Jenny's Story: My Life with Crouzon Syndrome
Growing Up with Crouzon Syndrome
Being an Adult with Crouzon Syndrome
Being a Mother with Crouzon Syndrome
Dealing with Unexpected Crouzon Syndrome
Helping Your Child to Cope with Teasing
~~~~~
Jenny's Inspirational Sayings II
~~~~~


The skull of an infant is made up of free-floating bones separated by fibres called sutures. This arrangement allows the infant's head to pass through the birth canal and also enables the skull to grow with the brain in early infancy. When a baby is born it has nearly 40 percent of his or her adult brain volume and this increases to 80 percent by three years of age. The baby's skull is also 40 percent of its adult size and by seven years this increases to 90 percent. Rapid growth occurs in the first three years.
Craniosynostosis:
Craniosynostosis is a medical word that means that one or more of the sutures of an infant's head have closed early (synostosis is the union of two or more bones to form a single bone). The sutures are the spaces between the bones that make up the skull. These sutures have each been given a name. See the picture below. Each of the skull bones also has a name and the fontanelles which are labelled on the diagram are known commonly as 'soft spots'.
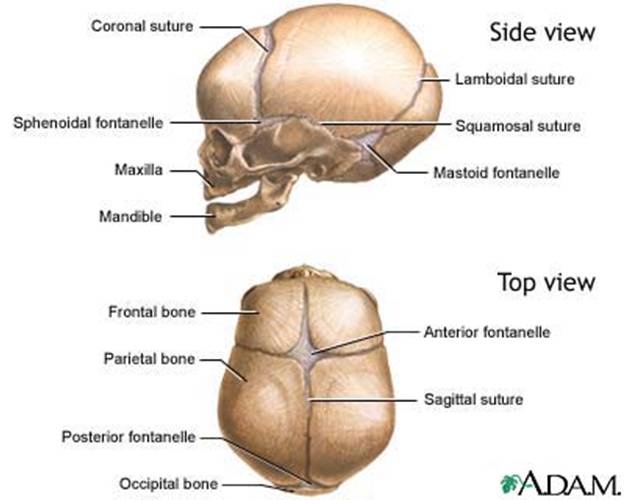
As an infant's brain grows the sutures allow the skull to expand and give room for the brain to grow. If one or more of the sutures has closed early, it causes the skull to expand in the direction of the open sutures. This can result in an abnormal head shape.
The cause of this premature fusion is unknown. Craniosynostosis is commonly present at birth but is not always noticeable, especially when mild. It often becomes more noticeable in the first few months of life. It can cause facial and cranial abnormalities and cause increased pressure on the growing brain which can have adverse effects on the child's development. A small minority of children present late. These children have mild deformity that is unnoticed in the first few months and years of life, and they present when aged 4-8 years with symptoms of raised intracranial pressure. The overall incidence of craniosynostosis is estimated as 1 case in 2000 live births.
There are many types of craniosynostosis. They are based on which suture or sutures are fused. The main types are described below:
Types of Craniosynostosis:
Scaphocephaly - Early fusion of the sagittal suture (from the Greek words scaphas, meaning boat, and kephalin, meaning head)
In scaphocephaly, the sagittal suture is closed. The sagittal suture runs from a spot at the front of the head to the back of the skulI. As a result, the infant's head does not expand in width but grows long and narrow to accommodate the growing brain. There may be bulging of the front and back of the head. The sagittal suture is the most common single suture involved in craniosynostosis. The incidence of sagittal synostosis in the population is approximately 1 in 4200 births. Males are affected about three times as often as females.
Surgery of sagittal craniosynostosis involves removing the suture and widening the skull by opening up the coronal and lambdoid sutures on both sides of the head. Sometimes bone grafts are placed to keep the out-fractured bones apart.
|
|
|
|

Plagiocephaly - Early fusion of one coronal suture (from the Greek word plagios, meaning oblique or sloping)
Anterior plagiocephaly (also known as unilateral coronal synostosis) - In plagiocephaly one of the coronal sutures are fused.
The coronal suture goes from ear to ear on the top of the head. Early closure of one side results in the forehead and orbital rim (eyebrow) having a flattened appearance on that side. This gives a "lop-sided" appearance which is also known as the "winking" effect. These features may also be more apparent when looking at the child in the mirror.
Surgery of plagiocephaly involves the removal of the
fused suture and the forehead and brow reshaped and brought forward to match the
other side. In addition, the cheek may also be brought forward to reposition the
eye socket.
Posterior plagiocephaly - Early closure of one lambdoid suture
The lamboid suturs is at the back of the skull. When it closes early it causes the back of the skull to be asymmetrical. Surgery which removes the fused suture and re-shapes the back of the skull is necessary.
|
|
|
|



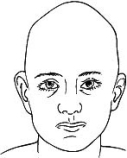
Brachycephaly - Early fusion of both coronal sutures (from the Greek word brachys, meaning short).
When both coronal sutures are fused it is called bilateral synostosis or brachycephaly. When this happens the baby may have a very flat, recessed high forehead. The head will be short and broad with bulging of the eyes and bulging of the skull around the ears. From side on the head will look squashed.
Brachycephaly is present in many craniofacial syndrome such as Crouzon, Pfeiffer, Saethre-Chotzen and Carpenters Syndrome.
To correct brachycephaly both fused sutures are removed and the skull is narrowed and lengthened. In addition, both cheekbones may be brought forward to reposition the eye socket.
|
|
|
|



Turricephaly - Early fusion of the coronal sutures (from the Latin word turris, meaning tall)
Turricephaly is a form of craniosynostosis that involves the bilateral fusion of the coronal sutures. The fusion gives a very tall and broad head with a narrow diameter.
|
|
|


Trigonocephaly - Early fusion of the metopic suture (from the Greek word trigonos, meaning triangular)
In trigonocephaly (also known as metopic synostosis) the metopic suture is fused. The metopic suture begins at the nose and continues up the forehead where it meets the sagittal suture. This results in a narrow, triangular shaped forehead. There is usually a ridge down the forehead that can be seen or felt and the eyebrows may appear "pinched" on either side. The eyes may also appear close together.
Surgery involves releasing the suture and expanding and rounding out the upper face, forehead and skull.
|
|
|
|

Oxycephaly - Early fusion of a combination of the bilateral coronal, sagittal, and sometimes lambdoid sutures (from the Greek word oxys, meaning sharp)
Oxycephaly is a form of craniosynostosis that involves the fusion of multiple sutures. The coronal, sagittal and lambdoid sutures are normally involved. This fusion gives a high, conical head with sharp bossing in the region of the anterior fontanelle
|
|
|

Kleeblattschadel or Cloverleaf skull - Early fusion of the coronal, lambdoid and psterior sagittal sutures or all of the sutures.
Premature fusion of the coronal, lambdoid and posterior sagittal sutures or all of the sutures can result in a rare condition known as cloverleaf skull (also known as kleeblattschadel). The fusion of the sutures gives the head a shape like a cloverleaf or a trefoil. Along with the fusion of the sutures comes a high forehead, severe bulging eyes (called proptosis, or exophthalmoses), a beaked nose and downward displacement of the ears. Hydrocephalus, multiple breathing and feeding issues may occur.
Surgery can give these babies a more normal appearing head.

Pansynostosis
Pansynostosis (also called complex multiple-suture synostosis) is the early fusion of multiple-sutures. These patterns of fusion do not conform to any of the other types. Complex multiple-suture synostosis is a mixture of otherwise unclassifiable combinations of affected sutures.
Not Craniosynostosis - Just a flattened head... - Positional Posterior Plagiocephaly
Not all abnormal head shapes are caused by craniosynostosis. Premature birth, restrictive intrauterine positioning, cervical abnormalities, birth trauma, torticollis (shortening of the neck muscle) and often sleeping positions can cause head shapes to be abnormal and for the skull to become flattened on one or both sides. This flattening of the head which is not due to fusion of the sutures is called positional moulding or positional plagiocephaly. Treatment includes repositioning the head, exercise and/or a corrective headband or helmet. It does not require surgical treatment.