

This site is under construction for a make over. Please excuse our mess.
This information is provided as a educational service by Organon Inc. and R. Jeffrey Chang, MD. While this web page provides this important information about PCOS and its treatment, it does not contain all the possible precautions, side effects, warnings, contraindications, and interactions which may be associated with your drug treatment. Your physician should discuss your treatment and possible side effects. Be sure to discuss any questions that you may have with you doctor before beginning treatment.
Polycystic Ovary Syndrome (PCOS) is a medical condition in which women experience irregular or absent menstrual bleeding, increased hair growth, and difficulty becoming pregnant. In these women, the
ovaries are slightly enlarged and contain multiple small cyst. Thus, Polycystic Ovary Syndrome is comprised of several clinical features, each of which may be present to a greater or lesser degree. As a result, patients may seek medical advice to correct irregular
menstruation, eradicate excessive hair growth, or achieve pregnancy.
Some women have been found to have polycystic ovaries without
associated abnormalities of menstruation, hair growth, or fertility. These women do not have Polycystic Ovary Syndrome. Thus, not all women with polycystic ovaries have PCOS, but all women with PCOS have polycystic ovaries.
Normal Ovarian Function
Women have two ovaries; they are located in the pelvis alongside the uterus. Their main function are to release eggs and produce hormones (illustration.)
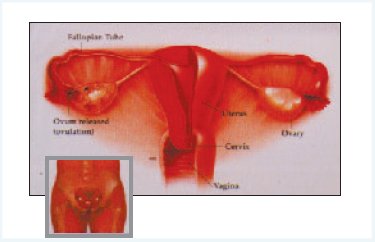
At birth the ovaries are provided with thousands of eggs, each surrounded by cells which develop into small fluid filled blister known as a follicle. Each month in women with regular periods (normal ovulation), one of the
follicles will develop and grow to about 20 mm in diameter and then release a mature egg (ovulation), which passes into the fallopian tub into the uterus where it will implant in the lining (endometrium) and develop as a pregnancy. If there is no fertilization, the endometrium is shed as a menstrual period around 14 days after ovulation.
Three important groups of hormones - estrogen, androgens, and
progesterone - are also produced in the ovary. There, in turn, are regulated by the release of two additional hormones; follicle-stimulating hormone (FSH) and luteinizing hormone (LH) from the pituitary gland which is located at the base of the brain. There two reproductive hormones influence the development of the follicle and the timing of ovulation.
Abnormal Ovarian Function - PCOS
Women with PCOS have normal reproductive organs such as the uterus and fallopian tubes. Their ovaries each usually contain about 10 or more small cyst located at the periphery of the ovary. The size of these cyst
generally are less then 8 mm and can be detected by ultrasound
examination. These cysts do not appear to grow and usually remain small. They do not require surgical removal. Additionally, these cyst do not represent cancer and are not associated with an increased risk of ovarian cancer.
The reason for multiple cyst development is not clear. It may be related to
the inability of ovulation in PCOS. In comparison to normal ovulation, a
woman with PCOS are unable to completely develop a fully mature egg (on
their own) due to abnormal pituitary FSH and LH secretion. As a result, the
ovulatory process is not completed and the partially stimulated follicle
becomes cystic followed by degeneration of the egg.
The problem of irregular or absent menstrual bleeding, excess hair growth
and infertility are a result of abnormal hormone secretion by pituitary gland
(FSH and LH) and the ovaries (estrogen, androgen and progesterone.)
Despite irregular ovulation in PCOS, the ovary continues to be stimulated
by FSH and LH in a uncoordinated manner, which leads to a constant
production of estrogen, excessive amounts of androgen, and very little
progesterone.
The Symptoms of PCOS
Menstrual Irregularities
Constant estrogen production stimulates growth of the uterine lining, or endometruim. As the lining grows and becomes abnormally thickened,there can be spontaneous shedding of the endometrium. This process, together with the lack of regular ovulation, leads to irregular and , sometimes, very heavy uterine bleeding. The bleeding episodes may occur after long gaps of time (oligomenerrhea) or, for some women, not at all (amenorrhea).
Impaired Fertility
Another consequence of incomplete follicular development is a lack of regular ovulation. Irregular ovulation usually means that pregnancy is more difficult to achieve. Similarly, if ovulation is not taking place, it is not possible to conceive. In most instances of PCOS, some form of treatment is necessary to re-establish predictable ovulation.
Miscarriage
While miscarriage seems an unfortunate chance event for most couples, it is now known that women with PCOS who have high circulating levels of LH may be at increased risk. A possible explanation is that levels of LH which are high in PCOS may interfere with the egg development within the follicle and/or disrupt embryo implantation within the uterus.
Hair and Skin Problems
Androgen (male hormone) is produced by ovaries from both normal women and those with PCOS. In PCOS the production of androgen, such as testosterone, is excessive, which causes abnormally increased hair growth and contributes to acne formation.
Obesity
About 50% of women with PCOS are obese. Obesity tends to enhance abnormal estrogen and androgen production in this disorder, which only madnifies the problems or irregular bleeding and excessive hair growth.
Abnormal Insulin Action
Recently, it has been discovered that is PCOS there is an abnormality of insulin secretion. Women with PCOS are more resistant to the action of insulin than normal women and, as a result, have a greater long-term risk of developing diabetes mellitus.
Heart Disease
Another long-term concern is that of cadiovascular risk. Androgens are known to induce an unfavorable lipid profile by increasing low density lipoprotein and decreasing high density lipoprotein. Thus, the excessive production of androgen in PCOS may place these women at an increased risk for heart disease.
Management of PCOS
Menstrual Irregularities
Irregular periods are a nuisance and suggest some hormonal disorder or risk of endometrial thickening. Any irregular bleeding should be checked by a doctor who may prescribe hormonal treatments to regulate the menstrual cycle.
Fertility Difficulty
In women with PCOS, failure to ovulate is the usual reason for not achieving pregnancy. However, prior to initiating fertility treatment, it is recommended that other factors which impact fertility should be evaluated. These factors include tubal patency, pelvic anatomic relationships, and assessment of semen and sprem function.
Monitoring Ovulation
In normal cycles, ovulation takes place 14 days before a period starts. For
instance, if your cycle is 28 days, ovulation will occur around day 14. If your
cycle is 27 days, ovulation will occur around day 13. If your cycle is 35
days, ovulation will occur approximately on day 21. It is important to
understand these relationships for the purpose of timing sexual intercourse
to coincide with ovulation. An inexpensive and convenient means by which
ovulation may be detected is using the basal body temperature (BBT) chart.
This methodology is based on the knowledge that a tempature rise of
approximately 0.5F occurs following ovulation and lasts for approximately
12 days. If ovulation does not occur or if the ovulation is faulty, then a rise
in temperature will be less then 11 days. It must be emphasized that
prediction of ovulation can only occur after several cycles of BBT have been
recorded.

Changes in the uterine lining in response to estrogen and progesterone.
A reasonably reliable way to predict ovulation is with an over the counter uninary test kit. This measures the surge of LH which occurs around the time of ovulation. Testing should begin a day or so before you expect to ovulate. Intercourse should take place on the day when there is a color change on the test, as well as on the following day.
Ovulation can be monitored by ultrasound, but this method is usually reserved for women having more complicated treatments, and for those who have difficulty with the urine test.
A blood test to measure circulating progesterone may be performed 7 days after presumed ovulation to determine whether ovulation has taken place. Progesterone is produced by the ovary following normal ovulation.
The efforts to monitor ovulation, whether simple or complicated, are intended to coordinate and the time sexual intercourse with that of ovulation. If there is a regular menstrual cycle and normal ovulation, then intercourse two or three times a weeks should provide a sufficient supply of sperm within the reproduction tract to maximize fertilization. It has been noted among patients that intensive monitoring can remove much of the spontaneity from their sex lives. Therefore, occasionally a short break from treatment, perhaps a month or two , might be considered to relieve the stress associated with this treatment.
Drugs to Induce Ovulation. In cases where ovulation is irregular or
absent, drugs can be used. The most common agent is clomiphene citrate,
which is taken as a tablet for five days from the third day of menstruation.
Results show that four out of five women given clomiphene do ovulate, but
only about one in three actually become pregnant. The starting daily dose
is usually 50 mg , which may be progressively increased up to a dose of 150 mg.
While clomiphene is a useful drug for many women with anovulation and
infertility, there are patients who fail therapy. If clomid has been unsuccessful
in women over six months of treatment, then alternatives therapies are usually
considered.
Side effects of clomid have been reported. These include stomach and bowel
upset, bloating, headaches, sensitivity to bright light, dizziness, hot flashes,
depression, and breast discomfort. Mild to moderate cystic enlargement of the
ovary may occur with clomid which necessitates discontinuance of the drug
and observation. Multiple pregnancy is slightly increased in women using this
form of ovulation induction. There is no increased risk of birth defects from clomid.
More complicated treatments. If clomid fails to successfully induce ovulation,
then a group of injectable hormone preparations. known as gonadotropins,
may be employed. There are two types of gonadotropin preparations available.
One contains both FSH and LH activities while the other contains primarily
FSH with a small amount of LH. Although both types of gonadotropins work
well in women with PCOS many programs prefer to use the products which
contains primarily FSH. Initial therapy includes daily administration in small
amounts with progressive increases in dose until ovulation is achieved.
Follicular development and growth is carefully monitored by hormone
measurements and ultrasound examinations. If monitoring shows that to many
follicles are developing, and risk of multiple pregnancy is high then treatment
will usually be suspended and ovulation induction in the cycle canceled. Then
development and growth of the follicle reaches optimum maturity, then human
chorionic gonadotropin (hCG) is administered by injection to stimulate release
of the egg from the follicle.
Women with PCOS given gonadotropins are at an increased risk of a rare
potentially serious condition know as Ovarian Hyperstimulation Syndrome.
This situation arises if an excessive number of follicles are stimulated. The
diagnosis is suspected when unusually large ovarian cyst formation occurs.
Avoidance of Ovarian Hyperstimulation Syndrome is best achieved by careful
monitoring of ovulation induction.
Ovarian Capsule Puncture Recently, it has been shown that
women with PCOS, penetration of the ovarian capsule by multiple puncture
results in resumption of regular ovulatory function. This is usually performed
through a laparoscope and puncture may be achieved by either cautery or
needle penetration at multiple sites. In some cases, regular ovulation persists
for some time, whereas in other patients, after several spontaneous normal
ovulations, irregular of absent menstrual function recurs.
In Vitro Fertilization (IVF)
The technique of IVF refers to the fertilization of a womans edd with her partners sperm in the laboratory. Following fertilization, the embryo is then placed in the womans uterus in anticipation of implantation and pregnancy. This procedure is recommended to women who have blocked fallopian tubes, or men with poor quality sperm. IVF is also offered to women with PCOS who wish to conceive after other treatment strategies have failed. Since a part of the protocol for IFV includes gonadotropin induction of ovulation, these patients must be carefully monitored in effort to avoid Ovarian Hyperstimulation Syndrome.
Summary
In summary, PCOS is the most common cause of menstrual irregularity in reproductive-ages women and its occurrence may be associated with a variety of clinical symptoms, including infertility. There are known long-term health risks associated with PCOS. As a result, patients with this condition are encourages to seek medical assistance since current therapies exist, which may prove to be extremely beneficial.
Please keep in mind you don't have to have all these symptoms, one or more is all you need to have PCOS.
**Amenorrhea ~ Meaning no menstrual periods, infrequent menstrual periods
and or irregular bleeding. Menstrual cycles are often more than six weeks
in length, with eight or fewer periods in a year. Irregular bleeding may include
lengthy bleeding episodes, scant or heavy periods, or frequent spotting.
** Anovulation ~Meaning infrequent or absent ovulation. Typically women
with PCOS produce follicles (fluid filled sacs on the ovary that contain the
egg). However the follicles often do not mature and do not get released as
needed for ovulation. It is these immature follicles that create the cysts.
** Hyperandrogenism ~ Meaning increased blood levels of male hormones. Specifically testosterone, androstenedione, and dehydroepiandrosterone (DHEAS).
** Infertility ~ Meaning the inability to get pregnant within six to twelve
months of unprotected sex,depending upon age. Concerning PCOS,
infertility is usually due to ovulatory dysfunction.
** Cystic Ovaries ~Classic PCOS ovaries have a "string of pearls" or
"pearl necklace" appearance with many cysts (fluid filled sacs). Alot of
PCOS women have enlarged ovaries with some cysts. But I stress you do
NOT need to have cysts on your ovaries to have PCOS. Some cysts may not
be recognized or noted by an ultrasonographer as they may not be recognized
as abnormal.
** Enlarged Ovaries ~ Polycystic ovaries are usually 1.5 to 3
times larger than normal.
** Chronic Pelvic Pain ~ Some PCOS women suffer chronic(happening
more than six months) pain in the pelvic area. It is not known what
exactly causes it, it has been suggested it may have be result of enlarged
ovaries or pelvic crowding.
** Obesity or weight gain ~ Women with PCOS topically have an "Apple
Figure", which is where weight is concentrated heavily in the abdomen.
It is similar to the way men often gain weight with comparably narrower
arms and legs. There is less difference between hip and waist
measurements. However please note NOT ALL women with
PCOS are overweight.
** Insulin Resistance, Hyperinsulinemia, and Diabetes ~ Insulin resistance
is a condition where a body's use of insulin is inefficient. Usually what
happens is that the body over produces insulin. This usually occurs with
normal glucose levels, however it may lead to diabetes where your bodies
tolerance to glucose goes down and the glucose in your blood may go up.
** Dyslipidemia ~ Meaning lipid abnormalities. Some women with PCOS
have elevated LDL and reduced HDL cholesterol levels and well as
high triglycerides.
** Hypertension Meaning high blood pressure. Blood pressure readings
over 140/90 is the usual area for concern.
** Hirsutism ~ Meaning excess hair. Excess hair growth such as on
the face, chest, abdomen, thumbs or toes are most common.
** Alopecia ~ Meaning male pattern baldness or thinning. The balding
is more common on top of the head than at the temples.
** Acne/Oily Skin/Seborrhea ~ Oil production is stimulated by
overproduction of androgens (male hormones). Seborrhea is
dandruff-flaking skin on the scalp caused by excess oil.
** Acanthosis nigricans ~ Meaning dark patches of skin, tan to dark
brown/black. Most commonly on the back of the neck, but also in skin
creases under arms, breasts, and between thighs, occasionally on the
hands, elbows and knees. The darkened skin is usually velvety or
rough to the touch.
** Acrochordons ~ Meaning tiny flaps (tags)of skin that usually
cause no symptoms unless irritated by rubbing.
Question about ovulation? Please check out the Ovulation Page!
It helps explain reason why women with PCOS do not ovulate.
If you would like to learn more on PCOS please feel free to join PCOS 2000. We are a group of women who are going through the same situation.
Click here to visit our wegpage, and to join.

Looking for good PCOS links? If so check out our links page.
We have put sites we find useful to use on this page for easy access.

If you would like to join our PCOS 2000 webring click here.
Check out the new message board!






Please check out the awards we have one!
To print a copy of the info from the booklet go to:
http://www.myfertility.ca/PDF/PO_book.pdf#search='Organon%20Inc.%20and%20R.%20Jeffrey%20Chang
|